COVID-19 rapidly accelerated the need for healthcare providers, payers, and patients to adopt digital services and interact in new, creative ways. Immediately after the lockdown announcement in March, the Indian Ministry of Health and Family Welfare issued the Telemedicine Practice Guidelines, which prompted greater confidence in virtual services.[1] In the US, the percentage of consumers using telehealth rose from 11% in 2019 to 46% by spring 2020, as patients scrambled to reschedule cancelled in-person visits.[2] At LABS, we knew we needed to shift our approach and meet our patients where we could: on their phones.
We piloted virtual support groups for patients who are enrolled in our programs and living with diabetes and hypertension.
· Prerna: With our regular group meetings on pause, we initially set up WhatsApp groups and conference calls to deliver accurate and timely COVID-19 information to members. As lockdowns persisted, we began to introduce topics from our diabetes & hypertension management curriculum through these new virtual channels and have continued to deliver remote health education over the past 6 months.
· Empower Health: The need for patient engagement during this period of isolation sparked the Empower Health virtual support group pilot. We created 12 weeks of content to promote diabetes & hypertension education, encourage healthy lifestyle changes, and provide health and safety information regarding COVID-19. We then invited patients from across our partner health facilities to participate.
Through these groups, we’ve learned important lessons on how to meaningfully engage patients in a virtual setting.
1. Meet patients on platforms they already use. Some of our patients are new to connecting online. Leveraging a commonly used platform in the region reduces the burden on patients and encourages greater participation. For example, in India and Kenya, we are using WhatsApp; as we partnered with reach52 to pilot a similar model in the Philippines, we moved to Facebook Messenger.
“It’s only after the COVID outbreak that I have started using WhatsApp groups. There are two groups that I am a part of. One is the church group and the other one is the Prerna group.”
– Group Member
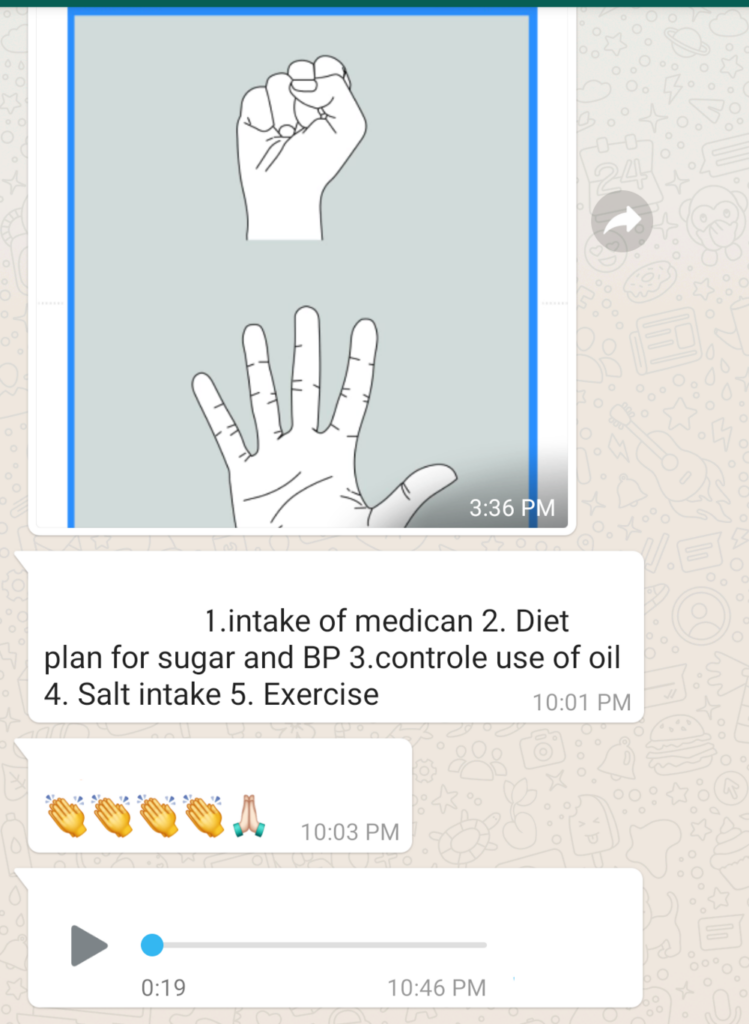
2. Use a variety of mediums to address the learning styles of all patients.
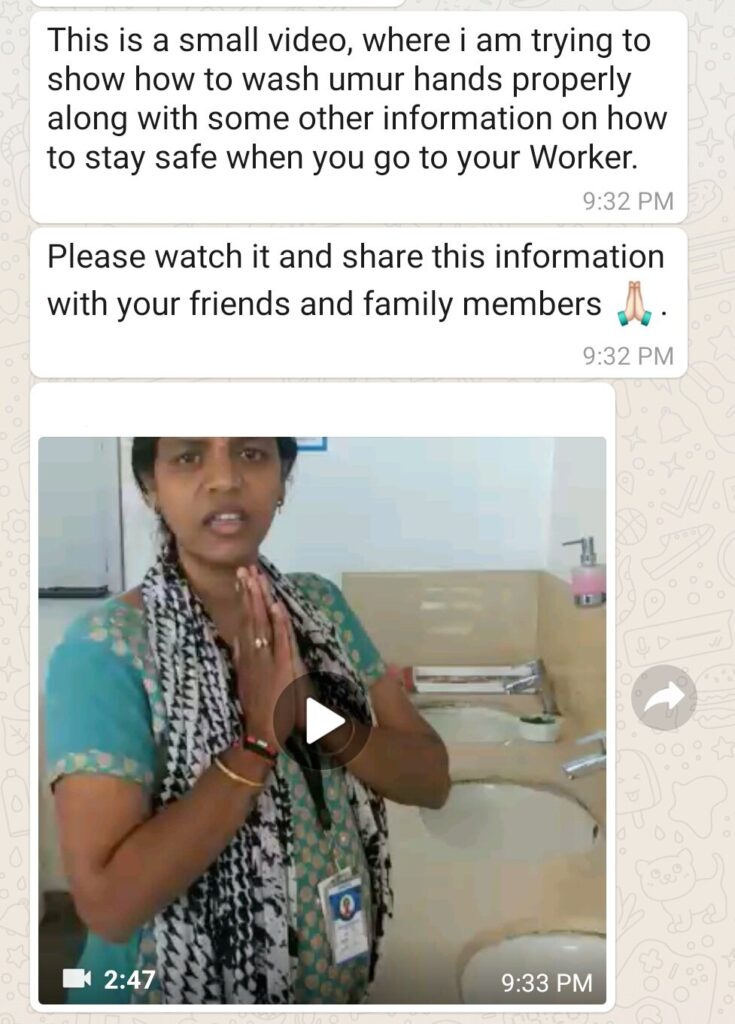
We share content via infographics, text, audio, and video messages. Patients reacted positively to audio and video recordings, which serve a dual purpose of reaching members of all literacy levels while creating a more personal connection to group facilitators and peers.
“I personally like the videos because they are easy to understand. I will give you an example: I like to cook. If I have to cook a new dish and you give me a recipe to read and cook, I will not be able to do it easily. But, if I see someone cooking, then I will quickly pick up all the details.”
– Group member

3. Facilitate peer-to-peer conversations to build community.
The power of groups comes from the opportunity to share challenges, learn from others, and provide encouragement. We use storytelling activities and crowdsource recommendations to promote conversation and relationship building among peers. This has been particularly important as we brought together Empower Health patients that had not met before. Our most popular prompt asked each member to share a link to a favorite song that helps them relax.
4. Recommend specific actions that promote a healthy lifestyle.
We implemented “Accountability Saturdays” to encourage members to add a healthy activity to their weekend routine and share it with the group. These activities included checking blood pressure and glucose levels, taking a 30-minute walk, and eating balanced meals. Members can send photos or texts about the activity for the group to celebrate weekly accomplishments.
5. Take creative approaches to reach patients without smartphones.
Only 25% of our current Prerna members have access to a smartphone. It is therefore imperative that we look for alternative ways to engage these patients. We’ve tested 1:1 tele-counseling calls as well as group conference calls, and we are currently working to translate our curriculum to SMS format.
By Lauren Leccese
[1] https://www.mohfw.gov.in/pdf/Telemedicine.pdf
[2] https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality